
Key Takeaways: How to Reduce Average Handle Time in Healthcare
-
1AHT in healthcare is structurally higher than other industries and that’s expected:
Clinical questions, insurance verification, triage decisions, and compliance requirements make healthcare calls inherently complex. The goal isn’t to hit retail benchmarks, it’s to eliminate preventable inefficiencies while preserving the quality of every patient interaction. -
2Never measure AHT as a single number across all call types:
Appointment scheduling, clinical triage, billing, and prescription refills have completely different natural handle times. Lumping them together produces meaningless averages. Segment by call type first, then set targets and identify improvement opportunities within each category. -
3Most AHT problems are training and workflow problems not technology problems:
Staff uncertainty about scheduling rules, insurance policies, and EHR navigation causes the majority of unnecessary hold time and prolonged conversations. A well-structured knowledge base and standardized call scripts address these before any technology investment is needed. -
4Hold time is the most fixable component of AHT:
Patients on hold waiting for staff to search records, confirm availability, or ask a nurse a question represent pure friction. Screen pop CTI integrations, pre-call data access, and structured triage protocols eliminate most hold time without changing anything about the conversation itself. -
5Reducing AHT while first-call resolution drops is not an improvement:
Shorter calls that push patients to call back, escalate, or visit in person cost far more than the handle time saved. FCR must be tracked alongside AHT at all times, it’s the guardrail that separates genuine efficiency from efficiency theatre. -
6AI and automation reduce wrap-up time at scale without touching clinical quality:
After-call documentation, EHR updates, referral scheduling, and follow-up instruction sending are all automatable. AI-assisted documentation can cut wrap-up time by 40–60% across thousands of calls, delivering significant AHT reduction without a single change to patient-facing conversation.
In today’s patient-centric environment, knowing how to reduce average handle time in healthcare is no longer just a call center concern, it’s a strategic priority. Average Handle Time (AHT) directly impacts patient access, staff workload, and operational efficiency across medical practices, hospitals, and specialty clinics.
Average handle time refers to the total time spent managing a patient interaction, from the moment a call is answered to the completion of documentation. In healthcare settings, this metric influences everything from appointment availability to front-desk stress levels and even patient satisfaction.
Unlike retail or general customer service industries, healthcare calls are inherently complex. Conversations often involve clinical nuances, emotional situations, insurance questions, compliance requirements, and triage decisions. These factors make healthcare call handle time naturally higher and more variable than other industries.
Still, high AHT can create long queues, abandoned calls, and burnout among medical receptionists and call center agents. Reducing average call duration in medical practices—without sacrificing safety or empathy can dramatically improve operational flow and patient experience.
This guide will walk you through:
- What AHT means in healthcare
- Common causes of long call times
- Practical strategies for improving call handling efficiency in healthcare
- Workflow, training, and technology improvements
- A step-by-step implementation roadmap
Let’s start with the fundamentals.
Table of Contents
Understanding Average Handle Time in Healthcare
What Is Average Handle Time (AHT)?

Average Handle Time (AHT) is calculated as:
Talk Time + Hold Time + Wrap-Up Time ÷ Total Calls
For healthcare phone interactions, this includes:
- Time speaking with the patient
- Time placing the patient on hold
- After-call documentation and administrative work
While AHT can also be calculated for chat and email channels, this article focuses specifically on phone calls because they remain the primary communication method in most healthcare organizations.
AHT Components in Healthcare Call Centers
1. Talk Time in Average Call Duration Medical Practices
Talk time includes:
- Verifying patient identity
- Scheduling appointments
- Answering insurance or billing questions
- Clinical triage discussions
- Explaining next steps
Talk time is often extended due to complex medical terminology, patient anxiety, or unclear scheduling protocols.
2. Hold Time in Healthcare Call Handle Time
Hold time occurs when staff:
- Search for patient records in the EHR
- Confirm provider availability
- Ask nurses for triage clarification
- Transfer to another department
Excessive hold time signals workflow friction and inefficient healthcare call routing strategies.
3. Wrap-Up Time
Wrap-up time includes:
- Documenting notes in EHR/PMS
- Sending follow-up instructions
- Scheduling referrals
- Updating insurance information
In healthcare, wrap-up time can be significant due to compliance and documentation standards.
AHT Benchmarks for Healthcare
Healthcare AHT varies by specialty and call type. General ranges often fall between 4–8 minutes for appointment calls and 8–15+ minutes for clinical triage or billing discussions.
However, a “good” AHT depends on:
- Outpatient vs high-acuity specialty clinics
- Patient population (elderly, chronic conditions, pediatrics)
- Call complexity
Healthcare organizations must define benchmarks by call category, not by a single universal number.
Why Reducing AHT in Healthcare Is Tricky (and Worth It)
Balancing Speed and Quality of Care
Lowering AHT should never compromise empathy or clinical accuracy. The goal is to improve call handling efficiency healthcare teams rely on while maintaining:
- First-call resolution in healthcare
- Patient satisfaction
- Clinical safety
Speed without resolution only shifts workload to callbacks and escalations.
Impact of High AHT on Operations
When handle times are long:
- Queue times increase
- Abandoned calls rise
- Front desk staff become overwhelmed
- In-clinic operations suffer
Long calls at the front desk reduce front-desk call efficiency, which spills into check-in delays and crowded waiting rooms.
Clinical Risk and Compliance Considerations
Some calls must remain longer:
- Symptom triage
- Medication clarification
- Post-procedure concerns
Standardized protocols help ensure calls are neither under-handled nor excessively prolonged.
Measuring AHT Correctly in Medical Settings
How to Calculate AHT in Healthcare Call Centers
Example:
If a clinic receives 500 calls in a week, and total talk + hold + wrap-up time equals 3,500 minutes:
3,500 ÷ 500 = 7 minutes AHT
Track AHT by:
- Appointment scheduling
- Clinical questions
- Billing
- Prescription refills
Segmentation reveals where improvements are needed.
Segmenting AHT by Call Type and Reason

Avoid lumping all calls together.
Differentiate:
- Scheduling vs nurse triage
- Billing vs refills
- New patient vs existing patient
Segmentation enables effective patient call workflow optimization.
Complementary Metrics: FCR, CSAT, and Abandonment
AHT must be analyzed alongside:
- First-Call Resolution (FCR)
- Customer Satisfaction (CSAT)
- Abandonment Rate
- Service Level
Optimizing AHT in isolation can damage patient experience.
Root Causes of Long Handle Time in Healthcare
Knowledge and Training Gaps for Medical Receptionists
Common delays occur when staff:
- Struggle with EHR navigation
- Don’t understand scheduling rules
- Are unsure about insurance policies
Improving medical receptionist call handling begins with training.
Inefficient Patient Call Workflows
Problems include:
- Duplicate data entry
- Unclear handoffs
- Overly complex scripts
Workflow confusion increases handle time dramatically.
Poor Healthcare Call Routing Strategies
Calls that bounce between departments inflate AHT and frustrate patients.
Intelligent routing ensures the right person handles the issue the first time.
Tool and System Friction
Slow EHR systems, multiple logins, and lack of integration add seconds to every action, which accumulates across thousands of calls.
Staffing and Environmental Factors
Understaffing, multitasking, and burnout increase both talk time and wrap-up time.
Training and Knowledge: The Foundation of Faster Calls
Invest in Role-Specific Call Representative Training
Train staff on:
- Scheduling protocols
- Insurance basics
- Clinical terminology
- EHR shortcuts
Regular refreshers reinforce efficiency.
Build a Medical Knowledge Base for Call Handlers
A strong knowledge base includes:
- Services and visit types
- FAQs
- Insurance policies
- Triage guidelines
This reduces hold time and improves first-call resolution.
Use Call Scripts and Scenario Playbooks
Scripts should guide—not restrict—conversations.
Create playbooks for:
- New patient intake
- Referrals
- Prescription refills
- Billing questions
Clear structure improves average call duration medical practices experience.
Coaching, Shadowing, and Call Reviews
Review recordings to:
- Identify unnecessary pauses
- Improve phrasing
- Share best practices
Top performers often provide replicable call handling techniques.
Patient Call Workflow Optimization
Map the End-to-End Patient Call Workflow
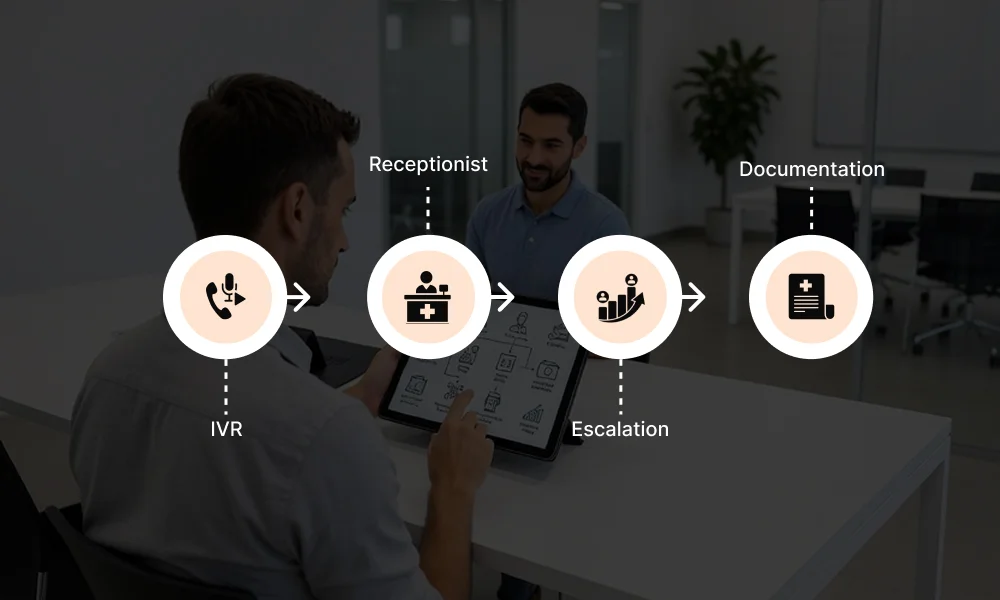
From IVR → receptionist → escalation → documentation.
Mapping exposes redundancy and inefficiencies.
Standardize Appointment Scheduling Workflows
Define:
- Visit types
- Slot lengths
- Provider matching rules
Pre-configured appointment types reduce back-and-forth.
Smart Triage Flows for Clinical Questions
Use structured protocols to:
- Classify urgency
- Route appropriately
- Document efficiently
This enhances call handling efficiency healthcare teams need.
Pre-Call Data and Screen Pops
CTI integrations can display patient information immediately, cutting search time significantly.
Healthcare Call Routing Strategies That Reduce AHT
Designing an Effective Call Routing Tree
Segment calls by:
- Appointments
- Clinical concerns
- Billing
- Referrals
Route directly to skilled teams.
Intelligent IVR and Self-Service Routing
Use IVR for:
- Hours
- Directions
- Basic FAQs
Avoid long menu trees.
Prioritizing High-Impact Calls
Skill-based routing sends complex calls to experienced agents, reducing transfers and improving first-call resolution healthcare benchmarks.
Leveraging Technology to Reduce Average Handle Time
Contact Center Tools: Call Recording, Monitoring, and Analytics
Dashboards tracking AHT by agent and call type reveal patterns and bottlenecks.
Knowledge Bases and In-Call Guidance
Embedded prompts shorten hold time and reduce errors.
Automation and AI Assistants
AI tools can:
- Handle routine questions
- Automate refill status checks
- Assist with documentation
AI-assisted note taking reduces wrap-up time.
Integrated Scheduling and Unified Systems
Unified EHR and scheduling platforms eliminate copy-paste inefficiencies.
Front-Desk Call Efficiency vs Dedicated Call Center
Front-Desk vs Centralized Call Center Models
Front desk staff multitasking between phones and patients often struggle with front-desk call efficiency.
Centralized teams improve consistency but require coordination.
Hybrid Models for Busy Practices
Peak-time routing to centralized teams protects in-clinic workflow.
After-hours outsourcing reduces missed calls.
Protecting Patient Experience While Lowering AHT

Reducing Dead Time, Not Patient Care
Cut:
- Silence
- Unnecessary holds
- Repeated questions
Keep meaningful clinical dialogue intact.
First-Call Resolution as a Guardrail
If FCR drops while AHT improves, efficiency gains are false.
Resolve issues completely on first contact whenever possible.
Setting Realistic Targets and Communicating Expectations
Set role-specific targets aligned with quality standards.
Review performance regularly.
Monitoring, Coaching, and Continuous Improvement
Building an AHT Performance Dashboard
Track:
- AHT by call reason
- FCR
- CSAT
- Abandonment
Identify patterns by time of day and provider schedule.
Feedback Loops With Agents and Clinicians
Regular meetings uncover workflow gaps and policy confusion.
Clinician input improves triage scripts.
Iterating on Workflows and Technology
Test improvements with small teams before scaling.
Continuous refinement drives sustainable improvement.
Implementation Roadmap: Applying These Strategies in Your Practice
30-Day Quick Wins
- Audit current AHT
- Segment call types
- Improve scripts
- Adjust routing
- Build a basic knowledge base
60–90 Day Optimization
- Deploy advanced contact center tools
- Integrate systems
- Formalize training
- Refine triage workflows
Long-Term Vision: Data-Driven, AI-Assisted Call Handling
Move toward:
- Predictive staffing
- AI-driven routing
- Automated documentation
Align call strategies with digital front-door initiatives.
Conclusion:
Learning how to reduce average handle time in healthcare is about more than shortening calls. It’s about eliminating inefficiencies while preserving empathy, safety, and resolution.
By combining:
- Targeted training
- Workflow optimization
- Intelligent healthcare call routing strategies
- Smart technology integration
Healthcare organizations can reduce average call duration in medical practices without sacrificing patient care.
When implemented strategically, AHT improvement becomes a competitive advantage, enhancing patient access, protecting staff wellbeing, and strengthening operational performance across the entire organization.
Frequently Asked Questions
What is average handle time (AHT) in healthcare?
Average handle time (AHT) is the total time spent managing a patient call, calculated as talk time plus hold time plus wrap-up documentation time, divided by total calls. In healthcare, AHT naturally runs higher than other industries due to clinical complexity, insurance verification requirements, and compliance documentation. Typical benchmarks are 4–8 minutes for scheduling and 8–15 minutes for triage or billing calls.
How do you calculate AHT in a medical practice?
Add total talk time, hold time, and wrap-up time across all calls in a defined period, then divide by the total number of calls. Always segment by call type scheduling, triage, billing, and refill calls have fundamentally different natural handle times, and mixing them produces benchmarks that mislead rather than guide improvement.
What causes high average handle time in healthcare?
The five most common causes are: staff knowledge gaps requiring holds to find answers, inefficient call workflows with redundant or unclear steps, poor call routing, sending patients to the wrong person or department, slow and fragmented EHR systems adding friction to every action, and understaffing that forces front desk staff to multitask between calls and in-person patients. Training and workflow standardisation address the majority of AHT problems before technology is needed.
What is a good average handle time for a healthcare practice?
4–8 minutes for routine appointment scheduling and 8–15 minutes for clinical triage or billing discussions are general industry benchmarks. The right target depends on your call mix, patient population, and specialty. More importantly, AHT should always be evaluated alongside the first-call resolution rate. A lower AHT that causes more callbacks is not an improvement.
How can medical practices reduce average handle time without reducing care quality?
The highest-impact steps are: build a centralised knowledge base so staff answer questions without placing patients on hold; standardise scheduling workflows and appointment types to eliminate back-and-forth; implement skill-based routing so each call type reaches the right person first time; use CTI screen pops to display patient records on call answer; and deploy AI assistants to handle routine enquiries and automate wrap-up documentation.
Should healthcare practices focus only on lowering AHT?
No AHT must be tracked alongside first-call resolution (FCR), patient satisfaction (CSAT), and abandonment rate. Reducing handle time while FCR drops means unresolved calls are just returning as callbacks or escalations, which costs more than the time saved. AHT improvement is only genuine when resolution quality and patient experience remain stable or improve simultaneously.
Want to Cut Call Handle Times Without Cutting Patient Care?
Book a call to see how MedLaunch helps clinics reduce average handle time through AI-powered call handling, automated wrap-up documentation, and smart routing.

